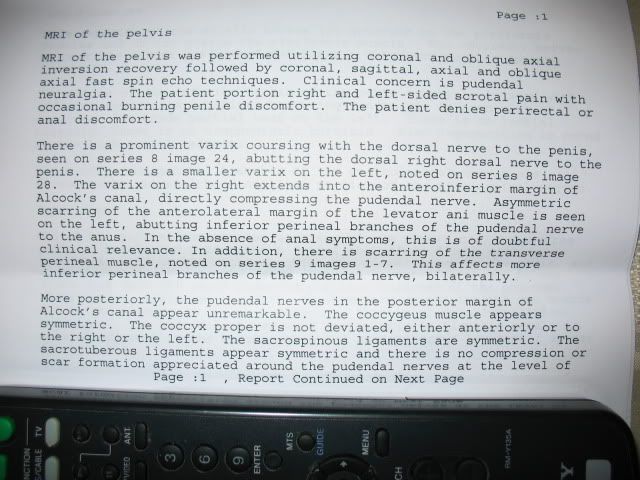
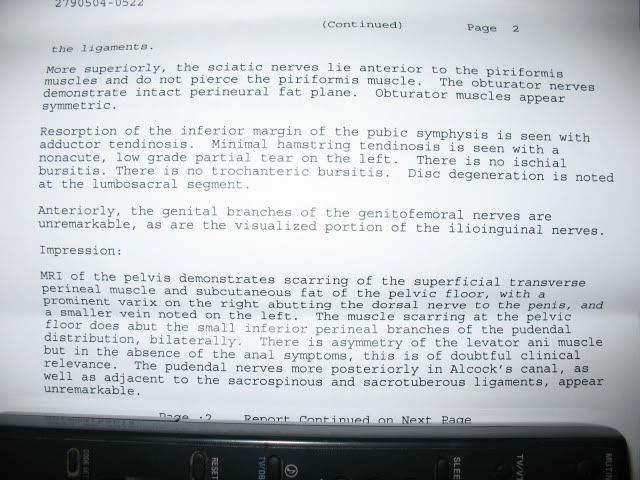
Page 1 of 4
MRI results from Dr. Potter visit
Posted: Sat May 28, 2011 5:17 pm
by PaulSa
Hello,
Just back from my visit to NY for an MRI with Dr. Potter. I will provide more details later if interested, just really sore right now from the flight and some sightseeing we did. I must say, the staff at HSS were very friendly and pleasant to deal with. Also had the pleasure of meeting and spending time with Dr. Potter and her assistant Nina to go over the results.
My home printer is not working right now so I took some pictures of the report to post. From what Dr. Potter said and what the images show I don't require surgery but I'm a little confused as to what I need to do to get rid of my condition? I will have to follow up with my pelvic floor specialist and Dr. Gordon. Please have a read and let me know your thoughts. It seems that the findings don't really match my symptoms I’m experiencing.
Re: MRI results from Dr. Potter visit
Posted: Sun May 29, 2011 2:59 am
by nyt
PaulSa, I don't know what you discussed with Dr. Potter and I'm not a medical doctor but here are some of my thoughts.
We don't know what the limit of detection of scar tissue is for the MRI so you might have scar tissue around the pudendal nerve, such as in the posterior aspect of the pudendal nerve, that just can't be seen. It is good news though that it appears that at least your pudendal nerve looks good until you get out to at the least the anterior portion of Alcock's canal and that it is really the branches of the pudendal nerve that appear to be the areas with scarring.
A varix is a dilated/swollen vein or artery. Since veins, arteries and nerves run together as a neurovascular bundle that evidence of a compressed nerve by scarring is a dilated vein because the vein is also compressed from the scarring. To me this suggest that you have some type of bilateral entrapment of the dorsal branch of the pudendal nerve since the report shows varices worse on the right then the left dorsal branch. This could easily explain the penile burning that you complain of. Do you have any ED symptoms (you don't have to answer if to personal).
The perineal nerve branches and one of its branches is the posterior pudendal nerve which innervates the scrotum (see picture below). It seems possible to me that what Dr. Potter describes in the anteriorlateral margin of the levator ani muscle would account for the scrotal pain that you describe. Another possibility, since you don't complain of rectal pain, is that you have referred pain. There is evidence in other nerve conditions that the pain signal travels back up through the nerve and to another site and that is where the pain is felt.
Tendinosis is not the same as tendinitis and is a chronic change to the tendon due to muscle tears. Treatment options are limited and I commented on this on Mulan's MRI so I won't here.
Good luck with your next step and glad the MRI has information to help you move forward.

- Pudendal nerve
- Pudendal nerve male.png (102.64 KiB) Viewed 6902 times
Re: MRI results from Dr. Potter visit
Posted: Sun May 29, 2011 3:32 pm
by PaulSa
nyt wrote:PaulSa, I don't know what you discussed with Dr. Potter and I'm not a medical doctor but here are some of my thoughts.
We don't know what the limit of detection of scar tissue is for the MRI so you might have scar tissue around the pudendal nerve, such as in the posterior aspect of the pudendal nerve, that just can't be seen. It is good news though that it appears that at least your pudendal nerve looks good until you get out to at the least the anterior portion of Alcock's canal and that it is really the branches of the pudendal nerve that appear to be the areas with scarring.
A varix is a dilated/swollen vein or artery. Since veins, arteries and nerves run together as a neurovascular bundle that evidence of a compressed nerve by scarring is a dilated vein because the vein is also compressed from the scarring. To me this suggest that you have some type of bilateral entrapment of the dorsal branch of the pudendal nerve since the report shows varices worse on the right then the left dorsal branch. This could easily explain the penile burning that you complain of. Do you have any ED symptoms (you don't have to answer if to personal).
The perineal nerve branches and one of its branches is the posterior pudendal nerve which innervates the scrotum (see picture below). It seems possible to me that what Dr. Potter describes in the anteriorlateral margin of the levator ani muscle would account for the scrotal pain that you describe. Another possibility, since you don't complain of rectal pain, is that you have referred pain. There is evidence in other nerve conditions that the pain signal travels back up through the nerve and to another site and that is where the pain is felt.
Tendinosis is not the same as tendinitis and is a chronic change to the tendon due to muscle tears. Treatment options are limited and I commented on this on Mulan's MRI so I won't here.
Good luck with your next step and glad the MRI has information to help you move forward.
Pudendal nerve male.png
Thanks for the insight NYT, some great information you provided.
Most of my problem, about 97% is bilateral burning/pain over the sit bones that radiates up to my waist and down to my scrotum (I’ve only had burning in my scrotum approx 6-8 times over the last 8 months) when sitting. Only recently, have I experienced burning in my penis (approximately 3 or 4 times) in the 4 years I’ve had this condition; so far, no issues with ED.
When you speak about “referred pain” is this similar to cross talk? If so, the Gabapentin seems to have almost eliminated all the hot flashes I was experiencing down both my legs.
You seem to know quite a bit! Any thoughts on if you think this could be corrected without surgery or working with a pelvic floor specialist? Her methods include both internal and external therapy.
Thanks again!
Re: MRI results from Dr. Potter visit
Posted: Sun May 29, 2011 5:13 pm
by nyt
Referred pain versus cross talk: Usually, when scientist refer to cross-talk they mean that different types of nerves communicate with each other via an electrical signal. For example, one type of sensory nerve communicating with another type of sensory nerve or a totally different class of nerves such as an astrocyte. Referred pain is when the pain originates in one area but felt in another. The classic example is someone with a heart attack might not feel it in their chest but as pain in their left arm.
You have nothing to loose when trying PT (see note below). It might be a good discussion to have with you dr. to see about treating your different tendinosis and hamstring tear. Below is a link to some very usual information on hamstring and adductor tendinosis as a starting point for your research. You might find that some of your pain at the ischial tuberosity is actually due to the hamstring tendinosis. If you get any relief from treating both your hamstring tendinosis and adductor tendinosis is well worth your time, effort and money. There should be a fair amount you can do on your own and these links will give you a good start for questions and treatment options.
http://www.livestrong.com/article/41252 ... endinosis/
http://www.proamsportsinjury.co.uk/addu ... injury.htm
http://depts.washington.edu/hhpccweb/ar ... linicID=10
In my humble opinion, when it comes to PT, no pain no gain is not what works for those of us with PNE. If you try internal work and it makes you worse, don't do it! If they give you exercises and they make you worse, stop! You know your body better than anyone else and if you try PT if what they are recommending is not working and makes you worse than either find a PT that will really listen and work with you or figure out on your own what works best for you.
There is no way that I can answer whether PT will cure you or fix you enough that you would not consider surgery. If the nerve is entrapped the way to unentrap the nerve is with surgery and there are no guarantees what your outcome will be with pudendal surgery. These are the tough decision we all individually struggle with. I can say though, getting the tendinosis under better control won't hurt you at all and that is something hopefully PT can do and if you decide you want to go the surgery route you will better off to have other problems under better management for a better outcome.
Re: MRI results from Dr. Potter visit
Posted: Tue Jun 07, 2011 9:08 am
by Pelvis Stressly
Just wanted to add a few points PaulSa...
1.) There's no existing evidence (that I know of anyway) that varices can cause compression of the PN. Potter saw similar varices in my scan & recommended embolization, but when I checked in on the subject w. my usual team of experts I got the following responses...
"There is no case series about the treatment of varices and pudendal neuropathies." Dr. Beco (PN doc)
"Veins are soft and do not compress nerves. Indeed, varicosities often develop when the nerve is decompresssed." Dr. Antolak (PN doc)
"There is no documentation that I have read that suggest that varices can press on the pudendal nerve." Carolyn Vandyken (pelvic floor PT)
"Pelvic floor varices might result in pain, but the type of pain has usually been described as a dull achy pain." Dr. Jarvi (urologist)
"Veins are generally low pressure and cause symptoms from compression in rare circumstances." Dr. Beecroft (interventional radiologist)
Needless to say, I decided against the procedure.
2.) It's possible to have arteriopathy (or other vascular issues) in the area without necessarily having any associated neuropathy. This was demonstrated in 2 studies by Shafik from the '90s (I can send you the links if you want to check them out). In them, he performs decompression surgery on patients w. pudendal arteriopathy (compressed pudendal artery), only some of whom also have associated neuropathy. So just because a vein is compressed, it doesn't automatically mean that PN is also necessarily involved.
Have you spoken w. Carolyn out in Cambridge (PT mentioned above) yet? She's really good...I would definitely suggest getting her 2 cents (on both Potter's report & just your situation in general).
Also, any luck w. the OHIP appeal you mentioned earlier?
Take care, PS.
Re: MRI results from Dr. Potter visit
Posted: Tue Jun 07, 2011 1:40 pm
by nyt
I agree that the likelihood of a varice compressing the nerve and causing PN is very unlikely because they are a low pressure system. What both Dr. Howard and Dr. Hibner told me that in their experience when they have seen dilated pudendal veins when they have done surgery they have found entrapped pudendal nerves. These dilated veins would be like taking a long balloon, filling it with water then tying a knot around the middle of balloon you will have bulges around the knot. That is what they think happens when there is scarring around the vein and since it is runs next to the pudendal nerve the assumption is made that the pudendal nerve is entrapped also.
I know someone else on the board where Dr. Potter saw varices and recommended a treatment for them, which she had done, and it did not help one bit. Personally, Dr. Potter is an outstanding radiologist but she can't keep up to date on other areas of medicine, no dr. can, so you should go to someone who specializes in the problem that shows up on the MRI and talk with them regarding the best treatment options. I know Dr. Potter saw something on my MRI and made a suggestion about what she thought caused it. I don't think she is right with her analysis of the cause because she just don't know enough about my medical history and once I'm recovered from this surgery I'm going to talk with my dr. about it.
Re: MRI results from Dr. Potter visit
Posted: Thu Jun 09, 2011 10:52 am
by Pelvis Stressly
Interesting re. Drs. H & H. It makes sense anatomically that there's often simultaneous compression on both the vessels & the nerve (as they all run so closely together). But all I was saying was that that isn't necessarily a given in all cases (as again, Shafik demonstrated in the '90s that it's possible to have a patient presenting w. a compressed pud. artery w.out any accompanying PN compression).
And agreed re. Potter. I know A's Mommy had an embolization done under her recommendation, but it didn't help (hence her subsequent surgery w. Hibner).
Good luck on your recovery!
PS
Re: MRI results from Dr. Potter visit
Posted: Thu Jun 09, 2011 1:30 pm
by Karyn
nyt wrote:I know someone else on the board where Dr. Potter saw varices and recommended a treatment for them, which she had done, and it did not help one bit. Personally, Dr. Potter is an outstanding radiologist but she can't keep up to date on other areas of medicine, no dr. can, so you should go to someone who specializes in the problem that shows up on the MRI and talk with them regarding the best treatment options. I know Dr. Potter saw something on my MRI and made a suggestion about what she thought caused it. I don't think she is right with her analysis of the cause because she just don't know enough about my medical history and once I'm recovered from this surgery I'm going to talk with my dr. about it
Pelvis Stressly wrote:And agreed re. Potter. I know A's Mommy had an embolization done under her recommendation, but it didn't help (hence her subsequent surgery w. Hibner).
I agree. Didn't she also recommend a venous embolization for someone else and injections (not PN blocks) for another person, to no avail?
Re: MRI results from Dr. Potter visit
Posted: Fri Jun 10, 2011 2:51 am
by PaulSa
Pelvis Stressly wrote:Just wanted to add a few points PaulSa...
1.) There's no existing evidence (that I know of anyway) that varices can cause compression of the PN. Potter saw similar varices in my scan & recommended embolization, but when I checked in on the subject w. my usual team of experts I got the following responses...
"There is no case series about the treatment of varices and pudendal neuropathies." Dr. Beco (PN doc)
"Veins are soft and do not compress nerves. Indeed, varicosities often develop when the nerve is decompresssed." Dr. Antolak (PN doc)
"There is no documentation that I have read that suggest that varices can press on the pudendal nerve." Carolyn Vandyken (pelvic floor PT)
"Pelvic floor varices might result in pain, but the type of pain has usually been described as a dull achy pain." Dr. Jarvi (urologist)
"Veins are generally low pressure and cause symptoms from compression in rare circumstances." Dr. Beecroft (interventional radiologist)
Needless to say, I decided against the procedure.
2.) It's possible to have arteriopathy (or other vascular issues) in the area without necessarily having any associated neuropathy. This was demonstrated in 2 studies by Shafik from the '90s (I can send you the links if you want to check them out). In them, he performs decompression surgery on patients w. pudendal arteriopathy (compressed pudendal artery), only some of whom also have associated neuropathy. So just because a vein is compressed, it doesn't automatically mean the PN is also necessarily involved.
Have you spoken w. Carolyn out in Cambridge (PT mentioned above) yet? She's really good...I would definitely suggest getting her 2 cents (on both Potter's report & just your situation in general).
Also, any luck w. the OHIP appeal you mentioned earlier?
Take care, PS.
I currently have an appointment with Dr.Gordon on the 13th, it will be interesting to see if he brings anything to the table. I'm currently working with Nelly Faghani who I believe is partners in crime with Carolyn. I also emailed Dr. Hibner's assistant Patty, she said he would be willing to have a look at my MRI which I emailed to him. She then emailed me to tell me he had a look and said he could help but said I needed to go down for a consult, I explained that I would be coming from Canada and just wanted to know if I was a candidate for surgery and that was that.
Just faxed in the paperwork a few days ago for the appeal and waiting to hear back for next steps. Thanks for all the great info.
Paul
Re: MRI results from Dr. Potter visit
Posted: Sat Jun 11, 2011 2:34 am
by RJR
Great discussion to all the above. Similar for me: Dr Potter did note prominent varix compressing the R pudendal nerve. At surgery Dr Hibner validated her finding, but did not ligate it because 1) felt it was no threat 2) possible ED.
...and nyt, thanks for the excellent links above. Best wishes on your recovery!
RR